Anatomic Pain Generators in the Shoulder: Unraveling the Sources of Discomfort

Shoulder pain can be a frustrating and debilitating issue, affecting everything from daily tasks to athletic performance. The shoulder’s complex anatomy, with its intricate network of bones, muscles, tendons, and ligaments, makes it prone to a variety of problems. Understanding the specific structures—or “pain generators”—that contribute to shoulder discomfort is key to effective diagnosis and treatment.
Today, we’ll explore the main anatomic pain generators in the shoulder, what causes them to flare up, and how they contribute to pain, all explained clearly for a general audience.
The Shoulder’s Complex Design
The shoulder is one of the body’s most mobile joints, allowing you to lift, throw, and rotate your arm with ease. This flexibility comes from a combination of structures working together:
- Bones: The humerus (upper arm bone), scapula (shoulder blade), and clavicle (collarbone).
- Joints: The glenohumeral joint (where the humerus meets the scapula), acromioclavicular (AC) joint (where the clavicle meets the scapula), and sternoclavicular joint.
- Soft Tissues: Muscles (like the rotator cuff), tendons, ligaments, cartilage (labrum), and bursae (fluid-filled sacs that reduce friction).
- Nerves and Blood Vessels: Supplying sensation and nourishment to the region.
When any of these structures become injured, inflamed, or degenerated, they can act as pain generators, causing discomfort that ranges from mild to severe. Let’s dive into the key culprits.
Common Anatomic Pain Generators in the Shoulder1. Rotator Cuff (Muscles and Tendons)
- What It Is: The rotator cuff is a group of four muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) and their tendons that stabilize the shoulder and enable arm movement.
- Why It Hurts: Pain arises from:
- Tendinitis: Inflammation from overuse, often in athletes or repetitive tasks (e.g., painting or lifting).
- Tears: Partial or complete tears from acute injury (like a fall) or chronic wear, common in people over 40.
- Impingement: The tendon gets pinched under the acromion (part of the scapula), causing pain with overhead motions.
- Symptoms: Dull ache in the shoulder, pain when lifting the arm, weakness, or nighttime discomfort.
- Prevalence: Rotator cuff issues affect about 20-30% of adults, with tears increasing with age, per a 2015 study in Journal of Shoulder and Elbow Surgery.
2. Subacromial Bursa
- What It Is: A small, fluid-filled sac that cushions the rotator cuff tendons and reduces friction under the acromion.
- Why It Hurts: Bursitis occurs when the bursa becomes inflamed, often due to repetitive overhead activities, impingement, or trauma. It can also accompany rotator cuff issues.
- Symptoms: Sharp pain with arm movement, especially reaching overhead or behind the back, and tenderness over the shoulder.
- Prevalence: Subacromial bursitis is a common cause of shoulder pain, often seen in 10-25% of patients with rotator cuff pathology, per a 2019 review in American Family Physician.
3. Glenohumeral Joint (Including Cartilage and Capsule)
- What It Is: The ball-and-socket joint where the humerus fits into the scapula’s shallow socket, lined with cartilage and surrounded by a joint capsule.
- Why It Hurts: Pain generators include:
- Osteoarthritis: Cartilage wear causes bone-on-bone friction, leading to stiffness and pain.
- Rheumatoid Arthritis: Autoimmune inflammation of the joint lining (synovium).
- Adhesive Capsulitis (Frozen Shoulder): The joint capsule tightens, restricting movement and causing pain, often in people aged 40-60 or after immobilization.
- Symptoms: Deep joint pain, stiffness, grinding sensations, or limited range of motion.
- Prevalence: Frozen shoulder affects 2-5% of the population, per a 2020 study in Journal of Orthopaedics, while osteoarthritis is common in older adults.
4. Labrum
- What It Is: A ring of cartilage around the glenoid (scapula’s socket) that deepens the joint and stabilizes the humerus.
- Why It Hurts: Labral tears (e.g., SLAP tears, affecting the biceps tendon attachment) occur from trauma (like a fall on an outstretched arm), repetitive overhead motions (e.g., pitching), or dislocations.
- Symptoms: Catching or locking sensations, pain with overhead or twisting motions, instability, or a “popping” sound.
- Prevalence: Labral tears are seen in 10-20% of shoulder pain cases, especially in athletes, per a 2017 study in Sports Medicine.
5. Acromioclavicular (AC) Joint
- What It Is: The joint connecting the clavicle to the acromion, stabilized by ligaments.
- Why It Hurts: Pain stems from:
- AC Joint Arthritis: Degeneration from wear or prior injuries.
- Sprains or Separations: Trauma (e.g., a fall or collision) stretches or tears ligaments, common in contact sports.
- Symptoms: Pain at the top of the shoulder, worsened by crossing the arm across the body or lifting weights.
- Prevalence: AC joint issues account for 10-15% of shoulder pain cases, per a 2018 review in Current Reviews in Musculoskeletal Medicine.
6. Biceps Tendon
- What It Is: The tendon connecting the biceps muscle to the shoulder, running through the front of the joint.
- Why It Hurts: Biceps tendinitis or tears result from overuse, impingement, or trauma, often alongside rotator cuff issues.
- Symptoms: Pain in the front of the shoulder, worse with lifting or pulling, and sometimes a “popeye” bulge if the tendon ruptures.
- Prevalence: Biceps tendinitis is seen in 5-10% of shoulder pain patients, often linked to rotator cuff pathology, per a 2021 study in Orthopedics.
7. Nerves (Brachial Plexus and Peripheral Nerves)
- What They Are: Nerves supplying sensation and motor function to the shoulder and arm.
- Why They Hurt: Nerve irritation or compression from trauma, inflammation, or cervical spine issues (e.g., herniated discs) can cause referred shoulder pain. Conditions like thoracic outlet syndrome or suprascapular nerve entrapment are less common but relevant.
- Symptoms: Burning, tingling, or radiating pain, sometimes with numbness or weakness.
- Prevalence: Nerve-related shoulder pain is less common but significant in 5-10% of cases, per a 2019 study in Pain Medicine.
8. Referred Pain (Non-Shoulder Sources)
- What It Is: Pain felt in the shoulder but originating elsewhere, such as the neck, heart, or organs.
- Why It Hurts: Cervical spine issues (e.g., herniated discs), heart conditions (e.g., angina), or gallbladder disease can mimic shoulder pain.
- Symptoms: Vague, aching pain, often with neck stiffness or systemic symptoms (e.g., shortness of breath for heart issues).
- Prevalence: Referred pain accounts for 5-15% of shoulder pain cases, per a 2020 review in American Journal of Medicine.
How Pain Generators Are Identified
Pinpointing the exact pain generator requires a thorough evaluation:
- Medical History: Details about the pain’s onset, activities, and prior injuries.
- Physical Exam: Tests like range-of-motion checks or palpation to isolate the source.
- Imaging: X-rays for bones, MRIs for soft tissues, or ultrasound for dynamic assessment.
- Diagnostic Injections: Injecting anesthetic into a suspected structure (e.g., subacromial space) can confirm it as the pain source if relief occurs.
For example, a 2022 study in Journal of Orthopaedic & Sports Physical Therapy emphasized that combining clinical tests with imaging improves diagnostic accuracy for rotator cuff and labral issues.
Managing Shoulder Pain Generators
Treatment depends on the specific pain generator but often starts with conservative measures:
- Rest and Activity Modification: Avoiding aggravating movements while maintaining gentle motion.
- Physical Therapy: Strengthening the rotator cuff, improving posture, or mobilizing a frozen shoulder.
- Medications: NSAIDs (e.g., ibuprofen) or oral steroids for inflammation.
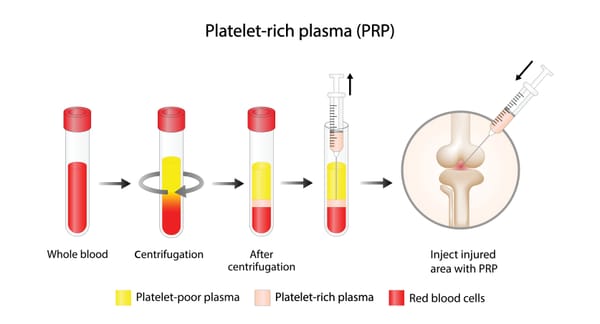
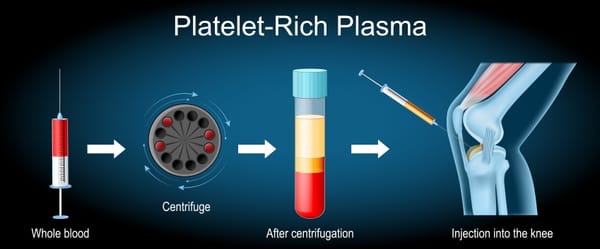
- Injections: Ultrasound-guided corticosteroid, hyaluronic acid, or platelet-rich plasma (PRP) injections to reduce pain or promote healing.
- Surgery: Reserved for severe cases (e.g., large rotator cuff tears or labral repairs) when non-surgical options fail.
For example, rotator cuff tendinitis may respond to physical therapy and a corticosteroid injection, while a complete tear might need arthroscopic repair.
A multidisciplinary approach, involving orthopedists, physical therapists, and pain specialists, is often most effective.Living with Shoulder Pain
Dealing with shoulder pain can feel isolating, especially when it limits your ability to work, play, or sleep. Understanding the pain generator empowers you to seek targeted treatment and advocate for yourself. Keep a symptom diary, ask your doctor about diagnostic tests, and explore support groups, like those through the Arthritis Foundation or online platforms like Reddit, to connect with others.Why Awareness Matters
Shoulder pain is common—affecting up to 25% of adults at some point, per a 2019 study in BMJ Open—but its causes are diverse. Recognizing the anatomic pain generators helps demystify the condition, leading to faster diagnoses and better outcomes. If you’re experiencing persistent shoulder pain, don’t ignore it.
Consult a healthcare provider to identify the source and start the right treatment plan.
By understanding the shoulder’s anatomy and its pain generators, we can take steps toward relief and support those affected. Let’s keep the conversation going—no one should shoulder their pain alone.
Disclaimer: This blog post is for informational purposes only and not a substitute for professional medical advice. Always consult a healthcare provider for diagnosis and treatment of shoulder pain.