Discogenic Lumbar Spine Pain: Understanding the Source and Finding Relief

Chronic lower back pain can be a frustrating and debilitating condition, and for many, the culprit lies within the spinal discs themselves—a condition known as discogenic lumbar spine pain.
This type of pain, originating from the intervertebral discs in the lower back, can significantly impact daily activities like sitting, standing, or even sleeping. Understanding discogenic pain is key to finding effective relief and improving quality of life. In this blog post, we’ll explore what discogenic lumbar spine pain is, its causes, symptoms, and treatment options, all explained clearly for a general audience.
What is Discogenic Lumbar Spine Pain?
Discogenic lumbar spine pain is chronic lower back pain caused by damage or degeneration in the intervertebral discs of the lumbar spine (L1-L5). These discs act as cushions between the vertebrae, absorbing shock and allowing flexibility. Each disc has a tough outer layer (annulus fibrosus) and a gel-like inner core (nucleus pulposus). When the disc is injured or degenerates, it can become a source of pain, either directly or by irritating nearby nerves.
Unlike pain from other sources like facet joints or muscles, discogenic pain is typically deep and centralized in the lower back. It’s estimated to account for 26-42% of chronic lower back pain cases, per a 2020 study in The Spine Journal, and is often challenging to diagnose due to its overlap with other conditions.
Causes of Discogenic Lumbar Spine Pain
Discogenic pain results from damage or changes in the intervertebral discs, triggered by various factors:
- Degenerative Disc Disease (DDD): Age-related wear and tear causes discs to lose hydration, height, and elasticity, leading to microtears or inflammation in the annulus.
- Disc Injury: Trauma from heavy lifting, falls, or accidents can cause tears in the annulus (annular tears) or disc bulging, irritating pain-sensitive fibers.
- Internal Disc Disruption (IDD): Microtears within the disc’s inner layers cause inflammation and pain without visible herniation.
- Herniated Disc: The nucleus pulposus bulges or ruptures through the annulus, sometimes pressing on nearby nerves, though discogenic pain is distinct from radicular pain (e.g., sciatica).
- Inflammation: Chemical irritation from damaged discs can inflame surrounding tissues or nerves.
- Repetitive Stress: Prolonged sitting, poor posture, or repetitive bending/lifting can strain discs over time.
Risk factors include aging (disc degeneration increases after age 30), obesity, sedentary lifestyles, smoking, or jobs involving heavy lifting or vibration exposure.
Symptoms of Discogenic Lumbar Spine Pain
Discogenic pain is characterized by symptoms distinct from other back pain conditions:
- Centralized Lower Back Pain: Deep, aching, or burning pain in the lower back, often without radiating to the legs.
- Pain with Movement: Worsened by sitting, bending forward, twisting, or lifting, as these increase disc pressure.
- Relief with Position Changes: Pain often eases when lying down, standing, or walking, which reduces disc stress.
- Stiffness: Limited flexibility in the lower back, especially after prolonged sitting.
- Occasional Radiating Pain: Mild discomfort may spread to the buttocks or hips, though not as far as the legs (unlike radiculopathy).
Symptoms can fluctuate, worsening with activity or stress, and may be accompanied by muscle spasms in the lower back. Discogenic pain rarely causes neurological symptoms like numbness or weakness unless a disc herniation compresses a nerve root.
Diagnosing Discogenic Lumbar Spine Pain
Diagnosing discogenic pain is challenging due to its overlap with other back conditions (e.g., facet joint pain, sacroiliac dysfunction). A thorough evaluation includes:
- Medical History: Discussing pain onset, location, triggers (e.g., sitting vs. standing), and history of trauma or degenerative conditions.
- Physical Exam: Testing range of motion, palpation for tenderness, and ruling out neurological deficits (e.g., weakness or numbness).
- Imaging:
- MRI: Visualizes disc degeneration, annular tears, or Modic changes (bone marrow changes linked to discogenic pain).
- X-rays: Assesses spinal alignment or arthritis but is less specific for discs.
- CT Scan: Used if MRI is unavailable to evaluate disc structure.
- Discography: A provocative test injecting contrast into the disc to confirm it as the pain source, though it’s controversial due to potential false positives.
- Diagnostic Injections: Facet or sacroiliac joint blocks to rule out other pain sources.
A 2021 study in Pain Medicine noted that combining MRI findings (e.g., high-intensity zones or Modic changes) with clinical symptoms improves diagnostic accuracy for discogenic pain by 80-85%.
Treatment Options for Discogenic Lumbar Spine Pain
Treatment focuses on reducing pain, improving function, and addressing disc inflammation or damage, starting with conservative approaches and escalating as needed.
1. Conservative Treatments
- Physical Therapy: Strengthening core and back muscles, improving posture, and using extension-based exercises to reduce disc pressure. Traction or manual therapy may help.
- Medications:
- NSAIDs (e.g., ibuprofen) for inflammation and pain.
- Muscle Relaxants for spasms.
- Neuropathic Drugs (e.g., gabapentin) for nerve-related pain.
- Oral Steroids for short-term relief of severe inflammation.
- Lifestyle Changes: Weight loss, ergonomic adjustments (e.g., lumbar support chairs), and avoiding prolonged sitting or heavy lifting.
- Activity Modification: Short-term rest followed by gradual return to activity to prevent deconditioning.
2. Interventional Procedures
- Epidural Steroid Injections or anesthetic discogram: Fluoroscopy- or ultrasound-guided injections to reduce inflammation around the disc. A 2020 study in Pain Physician found 50-60% of patients had relief for 1-3 months.
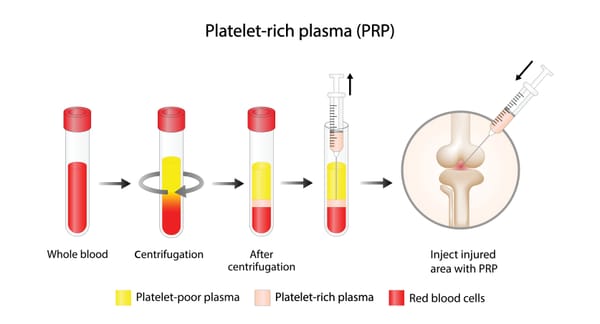
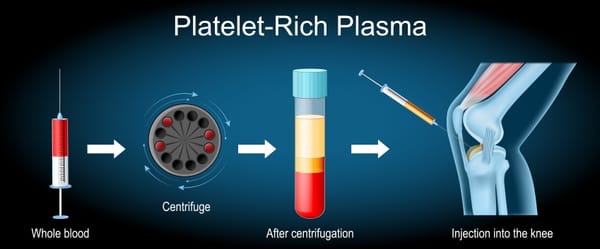
- Intradiscal Injections: Steroids or biologics (e.g., platelet-rich plasma, stem cells) injected into the disc.
- Radiofrequency Ablation: Targets pain-transmitting nerves (e.g., basivertebral nerve) for discogenic pain linked to endplate changes, per a 2021 study in The Spine Journal.
- Spinal Cord Stimulation: For chronic, unresponsive pain, implantable devices block pain signals.
- Minimimally invasive Discectomy (such as Disc-FX)
3. Surgical Treatments
- Discectomy: Removes part of a damaged disc, typically for herniations causing nerve compression, less common for pure discogenic pain.
- Spinal Fusion: Fuses vertebrae to stabilize the spine, used for severe disc degeneration or instability. A 2019 study in Spine reported 60-70% pain relief at 1 year.
- Artificial Disc Replacement: Replaces the damaged disc with a prosthetic, preserving motion. Less common but growing in use.
- Surgery is reserved for severe cases (5-10% of patients) after conservative treatments fail for 6-12 months or if neurological deficits occur.
4. Complementary Therapies
- Chiropractic Care: Gentle adjustments to improve spinal alignment, with caution to avoid aggravating the disc.
- Acupuncture: May reduce pain perception, with some studies showing benefits for chronic back pain.
- Psychological Support: Cognitive-behavioral therapy or mindfulness to manage chronic pain’s emotional toll.
A 2021 review in Global Spine Journal found that 60-70% of discogenic pain patients improve with conservative treatments within 3-6 months, with interventional or surgical options helping those with persistent symptoms.
Living with Discogenic Lumbar Spine Pain
Discogenic pain can feel isolating, limiting your ability to sit, work, or enjoy hobbies. Keep a pain diary to track symptoms and triggers, and share details with your healthcare team to guide treatment. Support groups, through organizations like Spine-Health (spine-health.com) or the North American Spine Society (spine.org), or online platforms like Reddit, offer a space to connect with others and share coping strategies.
Emotional support is crucial, as chronic pain can lead to stress or depression. Lean on counselors, family, or friends for encouragement. Practical steps, like using a lumbar support cushion, alternating sitting and standing, or practicing gentle stretches, can help manage symptoms.
Why Awareness Matters
Discogenic pain accounts for a significant portion of chronic lower back pain, yet it’s often misdiagnosed as facet joint pain, sacroiliac dysfunction, or muscle strain, per a 2020 study in Osteoarthritis and Cartilage. Raising awareness ensures patients receive accurate diagnoses and targeted treatments, preventing prolonged suffering.
If you’re experiencing chronic lower back pain, especially worsened by sitting or bending, consult a spine specialist, orthopedist, or pain management doctor to explore whether discogenic pain is the cause. Resources like Spine-Health or the American Academy of Orthopaedic Surgeons (aaos.org) offer valuable information and support.
By understanding discogenic lumbar spine pain, we can empower those affected to seek relief and reclaim their mobility. Let’s keep the conversation going—no one should face this pain alone.
Disclaimer: This blog post is for informational purposes only and not a substitute for professional medical advice. Consult a healthcare provider for diagnosis and treatment of discogenic lumbar spine pain.