Vertebral Augmentation for Vertebral Compression Fractures: A Minimally Invasive Path to Pain Relief
Vertebral compression fractures (VCFs) are a common and painful consequence of osteoporosis or other bone-weakening conditions, often causing significant back pain and reduced mobility. These fractures occur when a vertebra in the spine collapses, leading to discomfort that can severely impact quality of life. For those who find limited relief from conservative treatments like rest or medications, vertebral augmentation procedures—such as vertebroplasty and kyphoplasty—offer a minimally invasive solution to stabilize the spine and alleviate pain. In this blog post, we’ll explore what vertebral compression fractures are, how vertebral augmentation works, and what patients can expect, all explained clearly for a general audience.
Understanding Vertebral Compression Fractures
Vertebral compression fractures occur when one or more vertebrae, typically in the thoracic (mid-back, T1-T12) or lumbar (lower back, L1-L5) spine, collapse or crack due to weakened bone structure. They are most often linked to osteoporosis, a condition that reduces bone mineral density (BMD), making bones brittle and prone to fracturing under minimal stress, such as bending or lifting. Other causes include osteopenia, metastatic cancer, or multiple myeloma.
VCFs affect approximately 700,000 people annually in the U.S., with 20-30% of osteoporosis patients experiencing these fractures, per a 2020 study in Osteoporosis International. They can lead to chronic pain, height loss, spinal deformity (kyphosis), and reduced mobility, making effective treatment crucial.
Causes and Symptoms of Vertebral Compression Fractures
Causes include:
- Osteoporosis: The primary cause, with low BMD weakening vertebrae, especially in postmenopausal women due to estrogen decline.
- Osteopenia: Milder bone loss that can still lead to fractures.
- Pathologic Conditions: Bone metastases, multiple myeloma, or other cancers weakening the spine.
- Minimal Stress: Everyday activities like bending, lifting, or coughing can trigger fractures in fragile bones.
- Trauma: Minor falls in weakened bones, though less common.
Symptoms include:
- Sudden or Gradual Back Pain: Sharp or aching pain in the mid or lower back, worsened by movement or standing.
- Height Loss or Kyphosis: Vertebral collapse causes a hunched posture or reduced height.
- Reduced Mobility: Difficulty bending, twisting, or walking due to pain.
- Tenderness: Pain when pressing on the affected vertebra.
- Radiating Pain: Discomfort may spread to the ribs or abdomen, though rarely to the legs (unlike sciatica).
Up to 50-70% of VCFs are asymptomatic initially, per a 2020 study in The Lancet, often detected only after imaging, highlighting the need for targeted diagnosis.
What is Vertebral Augmentation?
Vertebral augmentation refers to minimally invasive procedures—primarily vertebroplasty and kyphoplasty—that stabilize VCFs by injecting bone cement (polymethylmethacrylate) into the fractured vertebra to relieve pain and restore structural integrity. Both procedures are performed under imaging guidance (fluoroscopy or CT) by interventional radiologists, pain specialists, or spine surgeons, typically outpatient or with a short hospital stay.
- Vertebroplasty: Involves injecting bone cement directly into the fractured vertebra to stabilize it.
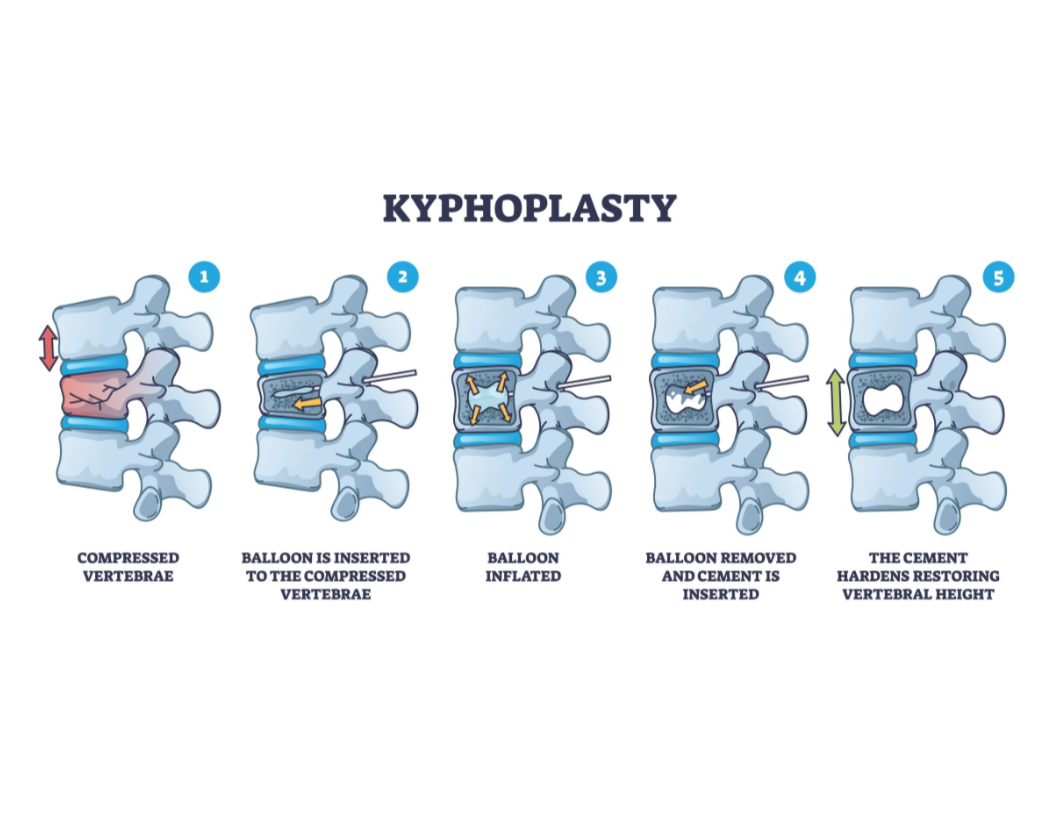
- Kyphoplasty: Uses a balloon to create a cavity in the vertebra before injecting cement, aiming to restore vertebral height and reduce deformity.
Both procedures take 30-60 minutes per vertebra under local anesthesia or mild sedation and are often considered when conservative treatments (e.g., pain medications, bracing) fail to provide relief after 4-6 weeks.
How Vertebral Augmentation Treats VCFs
Vertebral augmentation addresses VCFs by:
- Stabilizing the Fracture: Bone cement hardens quickly, reinforcing the vertebra and preventing painful movement.
- Relieving Pain: Stabilization reduces irritation of pain-sensitive nerves and surrounding tissues.
- Restoring Structure (Kyphoplasty): Balloon inflation may partially restore vertebral height, reducing kyphosis.
- Improving Mobility: Pain relief allows patients to resume daily activities more comfortably.
Vertebral augmentation is ideal for patients with:
- MRI- or CT-confirmed VCFs causing persistent pain.
- Pain unresponsive to 4-6 weeks of conservative treatments (e.g., rest, medications, bracing).
- Stable fractures without significant nerve compression or instability.
- Osteoporosis, osteopenia, or pathologic fractures (e.g., from cancer).
What Does the Evidence Say?
Research supports vertebral augmentation as an effective treatment for painful VCFs, particularly in osteoporosis. Key findings include:
- Pain Reduction: A 2020 meta-analysis in Pain Physician found that 70-80% of patients reported at least 50% pain reduction within 1-2 days post-vertebroplasty or kyphoplasty, with 65% maintaining relief at 6 months.
- Improved Function: A 2021 study in Journal of NeuroInterventional Surgery noted that 75% of patients had significant improvements in mobility and function (measured by the Oswestry Disability Index) at 3 months.
- Kyphoplasty Benefits: A 2019 study in The Spine Journal found that kyphoplasty restored vertebral height by 10-20% in 60% of patients, reducing kyphosis compared to vertebroplasty.
- Safety Profile: A 2020 review in Skeletal Radiology reported a low complication rate (<3%), with rare risks of cement leakage, infection, or adjacent fractures when performed with imaging guidance.
- Patient Experiences: On platforms like Reddit, patients describe vertebral augmentation as “a miracle,” with many regaining the ability to walk or sit comfortably, though some note temporary soreness or the need for ongoing osteoporosis treatment.
Vertebral augmentation is not a cure for osteoporosis, and new fractures may occur if the underlying condition is untreated. It’s less effective for unstable fractures, significant nerve compression, or non-osteoporotic causes.
What to Expect from Vertebral Augmentation
Here’s an overview of the process:
- Pre-Procedure: Your doctor will review your pain history, symptoms, and imaging (e.g., MRI or CT) to confirm a VCF. Blood tests (e.g., calcium, vitamin D) assess bone health, and a DEXA scan may confirm osteoporosis (T-score ≤ -2.5). You may need to stop blood thinners temporarily.
- Procedure:
- Vertebroplasty: A needle is inserted into the fractured vertebra under fluoroscopy or CT guidance, and bone cement is injected to stabilize it.
- Kyphoplasty: A balloon is inserted and inflated to create a cavity and restore height, followed by cement injection.
- The procedure takes 30-60 minutes per vertebra, usually outpatient under local anesthesia or mild sedation.
- Recovery: Most patients go home the same day. Mild soreness or bruising at the injection site is common for 3-7 days. Light activity can resume within days, with strenuous activity avoided for 4-6 weeks. Pain relief often begins within 1-2 days but may take 1-2 weeks to peak.
- Follow-Up: Regular check-ups with X-rays or CT monitor fracture healing and cement stability. Osteoporosis treatment is critical to prevent new fractures.
- Side Effects: Common side effects include temporary soreness or discomfort. Rare risks (<3%) include cement leakage, infection, or nerve irritation, minimized by imaging guidance and experienced providers.
Benefits and Considerations
Benefits:
- Significant pain relief, often 50-80% reduction, within days.
- Improved mobility and function, enabling better daily activities.
- Minimally invasive with a small needle puncture, low complication rate, and quick recovery.
- Stabilizes fractures, reducing risk of further collapse or deformity.
- Kyphoplasty may partially restore vertebral height, improving posture.
Considerations:
- Temporary side effects like soreness or bruising at the injection site.
- Rare risks include cement leakage, infection, or adjacent vertebral fractures (<3%).
- Costs range from $5,000-$15,000 per vertebra, with insurance coverage varying (often approved with confirmed VCFs and failed conservative treatments).
- Not suitable for unstable fractures, significant nerve compression, or non-osteoporotic causes.
- Requires ongoing osteoporosis treatment to prevent new fractures.
Is Vertebral Augmentation Right for You?
Vertebral augmentation is typically considered for patients with:
- MRI- or CT-confirmed VCFs causing persistent pain.
- Pain unresponsive to 4-6 weeks of conservative treatments (e.g., rest, bracing, medications).
- Stable fractures without significant spinal cord compression or instability.
- Osteoporosis, osteopenia, or pathologic fractures (e.g., from metastatic cancer).
Your healthcare team, including an interventional radiologist or pain specialist, will assess:
- The source of your pain, using imaging and clinical exams.
- Your overall health, including bone health and fracture risk (e.g., via DEXA scan or FRAX tool).
- Your goals, such as pain relief, improved mobility, or avoiding open surgery.
Discuss the procedure’s risks, benefits, and expected outcomes with your provider. Choosing a center experienced in vertebral augmentation is crucial for safety and success.
Complementary Treatments
Vertebral augmentation is often part of a broader management plan, including:
- Osteoporosis Treatment:
- Medications: Bisphosphonates (e.g., alendronate), parathyroid analogues (e.g., teriparatide), or denosumab to improve BMD and prevent fractures.
- Lifestyle Changes: 1,000-1,200 mg calcium and 800-1,000 IU vitamin D daily, weight-bearing exercise, and smoking cessation.
- Physical Therapy: Gentle exercises to restore mobility and strength, focusing on balance to prevent falls.
- Pain Management: NSAIDs, acetaminophen, or nerve blocks for residual pain.
- Fall Prevention: Home safety modifications (e.g., grab bars) or assistive devices like walkers.
- Psychological Support: Counseling or mindfulness to address pain’s emotional toll.
A 2021 study in Osteoporosis International found that combining vertebral augmentation with osteoporosis treatment reduced subsequent fracture risk by 40-50%.
Living with Vertebral Compression Fractures
VCFs can cause significant pain, height loss, or mobility issues, affecting daily life. Vertebral augmentation offers hope for relief, but addressing osteoporosis is key to preventing new fractures. Keep a record of pain, mobility issues, or falls, and share details with your healthcare team. Support groups, through organizations like the National Osteoporosis Foundation (nof.org) or online platforms like Reddit, provide a space to connect with others and share coping strategies.
Emotional support is vital, as pain and fear of fractures can lead to anxiety or reduced activity. Lean on counselors, family, or friends for encouragement. Practical steps, like using a back brace, installing grab bars, or practicing balance exercises, can reduce fracture risk and improve confidence.
Why Awareness Matters
VCFs affect 700,000 people annually in the U.S., with many remaining undiagnosed due to their silent nature, per a 2020 review in Osteoporosis International. Vertebral augmentation is a highly effective but underutilized treatment for painful fractures. Raising awareness ensures patients access this option when conservative treatments fail, improving outcomes and quality of life.
If you’re experiencing unexplained back pain, height loss, or have osteoporosis risk factors, consult an interventional radiologist, pain specialist, or orthopedist about vertebral augmentation. Resources like the National Osteoporosis Foundation (nof.org) or the International Osteoporosis Foundation (iofbonehealth.org) offer valuable information and support.
By spotlighting treatments like vertebral augmentation, we can bring hope and relief to those facing vertebral compression fractures. Let’s keep the conversation going—no one should endure this pain alone.
Disclaimer: This blog post is for informational purposes only and not a substitute for professional medical advice. Consult a healthcare provider for diagnosis and treatment of vertebral compression fractures or osteoporosis.